Left Atrial Appendage Isolation with Vein of Marshall Ethanol Infusion: Acute Procedural Success and Remapping
Purpose: Although the benefits of catheter ablation (CA) in atrial fibrillation (AF) are well established, patients with persistent AF often have high recurrence rates. While clinical trials have shown unclear benefits for posterior wall isolation, randomized trials have shown benefits for both Vein of Marshall (VOM) ethanol infusion and left atrial appendage isolation (LAAI) independently. LAAI is often challenging due to epicardial insertions from Bachman’s bundle and the coronary sinus. We hypothesize that VOM ethanol infusion coupled with anterior and lateral mitral lines to facilitate LAAI is a feasible and efficacious strategy for treating persistent AF.
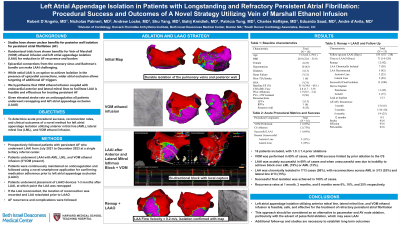
Material and Methods: We prospectively followed patients with persistent AF who underwent LAAI from July 2021 to December 2023 at a single tertiary referral center. Patients underwent left atrial appendage isolation with AML, LML, and VOM ethanol infusion (if possible). Patients underwent placement of left atrial appendage occlusion devices (LAAO) 1-3 months after LAAI, at which point the LAA was remapped. If the LAA had reconnected, the location of reconnection was recorded and the LAA was reisolated prior to LAAO.
Results: 16 patients were included, with average age 71.5 8.4, BMI 28.9 7.0, EF 51.4% 15.8 and CHADS2Vasc 2.8 1.1. Patients had undergone 1.9 1.4 prior ablations. The posterior wall and pulmonary veins were chronically isolated in 56% of patients who underwent LAAI. VOM was performed in 69% of cases, with VOM success limited by prior ablation to the CS. LAAI was acutely successful in 69% of cases and when unsuccessful was due to inability to achieve block over the lateral line (19%) or anterior line (13%). 13 patients underwent remapping at median 2.6 months post LAAI. LAA was chronically isolated in 7/13 cases (58%), with reconnections across the anterior line in 3/13 (25%) and lateral line 2/13 (29%). Successful final isolation was achieved in 100% of cases.
Conclusions: Left atrial appendage isolation utilizing anterior mitral line, lateral mitral line, and VOM ethanol infusion is feasible and safe for the treatment of refractory persistent AF. Additional follow-up and studies are necessary to establish long term outcomes, particularly as an alternative to pacemaker and AV node ablation.